
























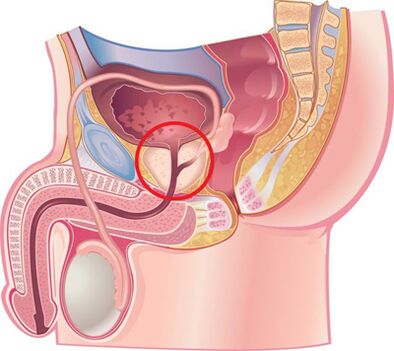
According to many experts, chronic prostatitis is an inflammatory disease caused by an infection with possible increase of autoimmune disorders, characterized by damage to the parenchymal and interstitial tissues of the organ. The disease has been known to medicine since 1850, but even today it remains poorly understood and reacts poorly to treatment. Chronic bacterial (6-10%) and non-bacterial (80-90%) prostatitis are the most common and socially important inflammatory diseases in men, significantly reducing their quality of life. The disease is recorded mainly in middle-aged people and is often complicated by impaired copulatory and generative functions (decreased potency, infertility, etc. ). The disease is registered in men in 8 - 35% of cases between the ages of 20 and 40 years.
The cause of bacterial prostatitis is the pyogenic flora, which penetrates the gland through the urethra, or by the lymphogenic and hematogenous pathways. The etiology of chronic non-bacterial prostatitis and its pathogenesis remain unknown. It mainly affects men over the age of 50.
Reasons for the development of the disease
Chronic prostatitis is currently considered a polyetiological disease. There is an opinion that the disease arises as a result of the penetration of the infection into the prostate, and then the pathological process continues without his participation. A number of non-infectious factors contribute to this.
Infectious factors in the development of chronic prostatitis
In 90% of cases, pathogens enter the gland from the urethra, resulting in acute or chronic prostatitis. There have been cases of asymptomatic transport. The course of the disease is influenced by the state of defense of the human body and the biological properties of the pathogen. It is assumed that the transition from acute to chronic prostatitis occurs due to loss of tissue elasticity due to excessive production of fibrous tissue.
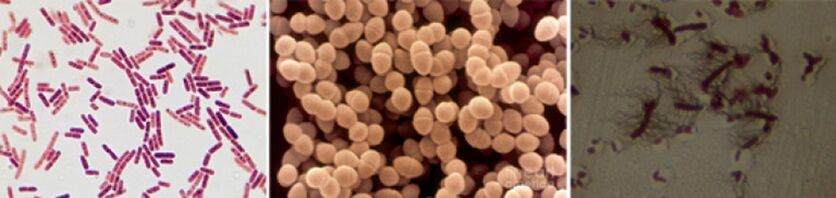
Among the causative agents of chronic prostatitis are the following pathogens:
- In 90% of cases, the disease detects such gram-negative bacteria as Escherichia coli (E. coli), Enterococcus faecalis (fecal enterococcus), somewhat less frequently - Pseudomonas aeruginosa, Klebsiella spp. , Proteus spp. , Pseudomonas aeruginogenes and Enterobacter. Gram-positive bacteria enterococci, streptococci and staphylococci are rare.
- The role of coagulase-negative staphylococci, ureaplasma, chlamydia, Trichomonas, gardnerella, anaerobic bacteria and fungi of the genus Candida has not been fully elucidated.
Infection enters the prostate in several ways:
- An ascending route is most likely, as evidenced by the frequent combination of prostatitis and urethritis.
- Hematogenous prostatitis develops when the infection penetrates the gland with the bloodstream, which is observed in chronic tonsillitis, sinusitis, periodontitis, pneumonia, cholecystitis and cholangitis, purulent skin diseases, etc.
- From contact, chronic prostatitis develops with urethritis and urethral constriction, when the infection enters the gland by adhering to the urine stream, with purulent kidney infections, by the canal route for epididymis, defrent and funicular, during diagnostic and therapeutic urological manipulations (catheter, urethralization), including transuretral.
- Lymphogenic infection crosses the prostate with proctitis, thrombophlebitis of hemorrhoidal veins, etc.
Non-infectious factors in the development of chronic prostatitis
Chemical factors
According to experts, the main role in the development of chronic prostatitis belongs to the intraprostatic reflux of urine, when urine is thrown from the urethra into the gland, which leads to damaged emptying of the prostate and seminal vesicles.
With the disease, vascular reactions develop, leading to edema of the organ, the nervous and humoral regulation of the smooth muscle tissue tone of the urethra is disturbed, the activation of alphaA- Adrenergic receptors cause the development of dynamic obstruction and contribute to the development of new intraprostatic reflux.
Bridges contained in urine, with reflux, lead to the development of an "inflammatory chemical response".
Hemodynamic disorders
They support chronic inflammation and circulatory disorders in the pelvic and scrotum organs. Overload develops in people who lead a sedentary lifestyle, for example, drivers, office workers, etc. , Overweight, sexual abstinence, sexual dysmetry, frequent hypothermia, mental and physical overload. Intake of spicy and spicy foods, alcohol and smoking, etc. , Contribute to the maintenance of the inflammatory process.
Other factors
There are many other factors that support chronic prostate inflammation. This includes:
- Hormonal.
- Biochemistry.
- Impaired immune response.
- Autoimmune mechanisms.
- Infectious and allergic processes.
- Characteristics of the structure of the prostate glands, leading to difficulty in complete drainage.
Often, the reasons for the development of chronic prostatitis can not be proven.
Classification of prostatitis
According to the classification proposed in 1995 by the National Institute of Health of SH. B. A. , prostatitis is divided into:
- Acute (category I). 5 is 5 - 10%.
- Chronic bacterial (category II). 6 is 6 - 10%.
- Chronic non-bacterial inflammation (category IIIA). 80 is 80 - 90%.
- Chronic non-bacterial non-inflammatory pain syndrome (category IIIB) or chronic pelvic pain.
- Chronic prostatitis, accidentally diagnosed (category IV).
Signs and symptoms of chronic prostatitis
The course of chronic prostatitis is long, but not monotonous. Periods of deterioration are replaced by periods of relative calm, which occur after complex anti-inflammatory and antibacterial therapy.
The development of chronic bacterial prostatitis is often preceded by urethritis of a bacterial or gonorrheal nature, non-bacterial - circulatory disorders of the pelvic and scrotal organs (hemorrhoids, varicocella, etc. ), sexual excess.
Patients with chronic prostatitis have many complaints. They go to doctors for years, but are rarely examined for prostate disease. About a quarter of patients do not present any complaints, or the disease persists with few clinical symptoms.
Complaints of patients with chronic prostatitis can be conditionally divided into several groups.
Urinary disorders associated with urethral stricture:
- Difficulty at the beginning of urination.
- Poor urine flow.
- Intermittent or point-to-point urination.
- Feeling of incomplete emptying of the bladder.
Symptoms due to irritation of nerve endings:
- Frequent urination.
- The desire to urinate is sharp and violent.
- Urination in small portions.
- Urinary incontinence during the urge to urinate.
Pain syndrome:
- The intensity and nature of the pain are different.
- Localization of pain: lower abdomen, perineum, rectum, groin and lower back, inner thighs.
Sexual dysfunction:
- Pain in the rectum and urethra during ejaculation.
- Slow erection.
- Loss of orgasm.
- Premature ejaculation, etc.
On the part of the nervous system: neurotic disorders in the form of fixing patients' attention to their state of health.
Signs and symptoms of chronic non-bacterial prostatitis
Chronic pelvic pain syndrome in men (CPPS) occurs with the usual symptoms of chronic prostatitis, but bacteria are absent in the 3rd part of the urine and in the secretion of the prostate gland. CPPS can be simulated from chronic non-bacterial interstitial cystitis, rectal diseases, spastic pelvic myalgic syndrome, and functional prostate lesions caused by disturbances in organ innervation and its hemodynamics.
If neurovegetative function is impaired, atony and a violation of the innervation of the gland, which is manifested by the difficulty of rapid and complete closure of the lumen of the urethra. At the same time, urine after urination continues to be excreted for a long time drop in points. In such patients, the study reveals increased instability and irritability, which is manifested by increased sweating and excitability of cardiac activity, changes in dermography.

Complications of the disease
The long course of chronic prostatitis is complicated by impaired sexual and reproductive functions, the development of diseases such as vesiculitis and epididymitis, as well as organ strengthening. Organ sclerosis worsens local microcirculation and urodynamics, as well as the results of surgical interventions. Periurethral tissue fibrosis leads to the development of urinary disorders.
Diagnosing
Due to the fact that there are many reasons for the development of chronic prostatitis, a whole range of diagnostic studies are used to diagnose it. The success of treatment depends on accurately determining the causes of the disease. The diagnosis of chronic prostatitis is based on the following data:
- The classic triad of symptoms.
- A set of physical methods (digital examination of the prostate colon).
- A set of laboratory methods (urine analysis and microscopy of prostate secretion, culture and determination of microflora sensitivity to antibacterial drugs, general analysis of urine and blood).
- For the detection of gonococci, bacterioscopy of urethral staining, PCR and serological methods (for the detection of ureaplasmas and chlamydia).
- Urofluometry.
- Prostate biopsy.
- Complex of instrumental methods (ultrasound).
- Determining the patient's immune status.
- Determination of neurological status.
- If treatment is ineffective and complications are suspected, magnetic resonance imaging and computer imaging, blood culture, etc.
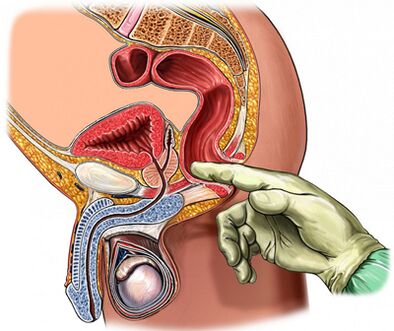
Palpation of the prostate
Of great importance in diagnosing the disease is palpation of the prostate, which increases during the period of deterioration and decreases during the period of reduction of the inflammatory process. In chronic prostatitis during an exacerbation of iron, it is edematous and painful.
The density of organ stability can be different: areas of softening and compression are palpated, areas of depressions are defined. On touch, it is possible to assess the shape of the gland, the condition of the seminal tubercles and the surrounding tissues.
The process of digital transrectal examination is combined with the collection of glandular secretion. Sometimes it becomes necessary to take the secret from each part separately.
Analysis of a 3-cup urine sample and prostate secretion
The "gold standard" in the diagnosis of chronic prostatitis are:
- Collection of the first part of urine.
- Collection of the second part of urine.
- Receiving glandular secretion by massage.
- Collection of the third part of urine.
Further, a microscopic and bacteriological examination of the material is performed.
With inflammation of the prostate:
- The number of microbes (CFU) exceeds 103/ ml (10four/ ml for epidermal staphylococci), but do not neglect the small number of microbes in the tens of hundreds.
- The presence of 10-15 leukocytes in the visual field, detected by microscopy, is a generally accepted criterion for the presence of an inflammatory process.
Prostate secretion and the third part of urine undergo microscopic and bacteriological examinations:
- In chronic bacterial prostatitis, there is an increase in the number of leukocytes in the secretion of the gland and the third part after the massage of the urine, the bacteria are released (mainly of the intestinal group).
- With non-bacterial prostate, there is an increase in the number of leukocytes in the secretion of the gland, but the microflora is not detected.
- With CPPS, there is no increased number of leukocytes and microflora.
Normal rate of prostate secretion:
- Leukocytes less than 10 in the visual field.
- There are many grains of lecithin.
- The microflora is missing.
In chronic prostatitis, prostate secretion reveals:
- The number of leukocytes is large - more than 10-15 in the field of view.
- The amount of lecine grains is reduced.
- The pH of the secretion shifts to the alkaline side.
- The acid phosphatase content decreases.
- Lysozyme activity increases.
Obtaining negative results of prostate secretion does not once prove the absence of an inflammatory process.
The value of the prostate secretion crystallization test is preserved. Normally, during crystallization, a characteristic pattern is formed in the form of a fern leaf. In case of violation of the accumulation properties of prostatic secretion, such a pattern is not formed, which occurs when the androgenic hormonal background changes.

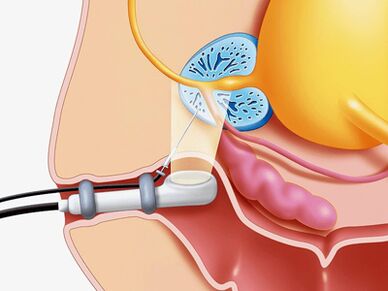
Ultrasound procedure
If a prostate disease is suspected, an ultrasound examination of the gland is used (transrectal ultrasound is optimal), kidneys and bladder, which makes it possible to determine:
- Gland volume and size.
- Presence of calculus.
- The size of the seminal vesicles.
- Condition of bladder walls.
- The amount of urine left.
- Scrotal structures.
- Another type of pathology.
Other prostate examination methods
- The state of urodynamics (a study of urine flow velocity) is easily and simply determined using a study such as uroflowmetry. With the help of this study, it is possible to detect in time the signs of blockage of the bladder outlet and perform a dynamic observation.
- Puncture biopsy is performed if abscess formation, benign hyperplasia, and prostate cancer are suspected.
- In order to clarify the reasons for the development of infravesicular obstruction, X-ray and endoscopic studies are performed.
- With a long-term inflammatory process, it is recommended to perform urethrocystoscopy.
Differential diagnosis
Chronic prostatitis should be distinguished from vesiculoprostatostasis, autonomic prostatopathy, congestive prostatitis, pelvic floor myalgia, neuropsychiatric disorders, pseudodinasinergy, reflex sympathetic dystrophy, inflammatory diseases of other organs: articular cystitis, interstitial cystitis, interstitial cystitis, interstitial cystitischronic epididymitis, inguinal hernia.
Chronic treatment of prostatitis
Treatment of chronic prostatitis should begin with changing the patient's lifestyle and diet.
In the treatment of the disease, drugs that affect different links of pathogenesis are used simultaneously.
Main directions of therapy:
- Elimination of causative microorganisms.
- Anti-inflammatory therapy.
- Normalize blood circulation to the prostate and pelvic organs.
- Normalize adequate drainage of prostatic acne.
- Normalization of hormonal profile.
- Prevention of organ strengthening.
For the treatment of chronic prostatitis, drugs of the following groups are used:
- Antibacterial.
- Anticholinergic.
- Vasodilators.
- AlphaA–Adrenergic blockers.
- 5 alpha reductase inhibitors.
- Cytokine inhibitors.
- Non-steroidal anti-inflammatory drugs.
- Angioprotectors.
- Immunomodulators.
- Drugs that affect urate metabolism.
Antibiotics in the treatment of chronic bacterial prostatitis
Antibiotic therapy should be performed taking into account the susceptibility of the identified microorganisms to antibiotics. If the pathogen is not identified, empirical antimicrobial treatment is used.
The drugs of choice are fluoroquinolones of generation II-IV. They penetrate quickly into the glandular tissues with the usual methods of application, are active against a large group of gram-negative microorganisms, as well as ureaplasma and chlamydia. In case of failure of antimicrobial treatment, it should be assumed:
- resistance to many microflora drugs,
- short courses (less than 4 weeks) of treatment,
- wrong choice of antibiotic and its dosage,
- changes in the type of pathogen,
- the presence of bacteria living in the prostate ducts, covered with an extracellular protective membrane.
The duration of treatment should be at least 4 weeks with mandatory subsequent bacteriological examination. If there is more than 10 bacteriuria in part 3 of urine and prostate secretion3CFU / ml, a repeated course of antibiotic therapy is prescribed for a period of 2 to 4 weeks.
Cytokine inhibitors in the treatment of chronic prostatitis
Cytokines are glycoproteins that are secreted by the immune system and other cells in response to an inflammatory response and an immune response. They take an active part in the development of the chronic inflammatory process.
Non-steroidal anti-inflammatory drugs
Non-steroidal anti-inflammatory drugs have anti-inflammatory effects, relieve pain and fever. They are widely used in the treatment of chronic prostatitis in the form of tablets and suppositories. The most effective way is colon administration.
Immunotherapy
In the treatment of chronic bacterial prostatitis, in addition to antibiotics and anti-inflammatory drugs, immunomodulatory agents are used. The most effective is the rectal route of their administration. An immunomodulator is widely used, which increases the functional activity of phagocytes, which contributes to a more efficient elimination of pathogens.
Alpha-blockers in the treatment of chronic prostatitis
Beenshte proved that alpha-1 adrenergic blockers normalize the smooth muscle tone of the prostate urethra, seminal vesicles and prostate capsule, which makes the drugs of this group very effective in treating the disease. Alpha-1 adrenergic blockers are used in patients with severe urinary disorders in the absence of an active inflammatory process.
With CPPS, the duration of treatment is 1 to 6 months.
5a-reductase inhibitor in the treatment of bacterial prostatitis and CPPS
It was found that under the influence of the enzyme 5a-reductase, testosterone is converted into the prostatic form 5a-dihydrotestosterone, whose activity in prostate cells is more than 5 times higher than the activity of testosterone itself, which in the elderly leads toan enlargement of the organ due to epithelial and stromal components.
When you take a 5a-reductase inhibitor for 3 months, stromal tissue atrophy is observed, within 6 months - gland, secretory function is inhibited, the severity of pain syndrome and gland volume is reduced, tension and edema of the organ are reduced.
The role of anti-sclerotic drugs in the treatment of chronic prostatitis
With prolonged inflammation in the prostate gland, fibrosis develops, which is manifested by impaired microcirculation and urodynamics. In order to prevent the process of fibrosis, anti-sclerotic drugs are used.
Other drugs used to treat chronic prostatitis
In addition to the drugs described above, the following are used to treat the disease:
- Antihistamines.
- Vasodilators and angioprotectors.
- Immunosuppressants.
- Drugs that affect the metabolism of urate and trisodium salt of citric acid.
Plant products
Effective in the treatment of prostatitis is the use of a preparation in the form of suppositories containing a complex of biologically active peptides isolated from the prostate gland of cattle.
Under the influence of the drug occurs:
- Stimulation of metabolic processes in glandular tissues.
- Improving microcirculation.
- Reduction of edema, leukocyte infiltration, secretion stagnation and pain.
- Prevention of thrombosis in prostate gland venules.
- Increased activity of the secretory epithelium of acin.
- Improving sexual function (increasing libido, restoring erectile function and normalizing spermatogenesis).
Prostate gland finger massage
A number of researchers argue that finger massage should be used for chronic prostate, given the known contraindications.
Physiotherapy
The effectiveness of physiotherapeutic procedures in the treatment of prostatitis has not been proven today, the mechanism of action has not been scientifically determined and side effects have not been studied.
Prevention of chronic prostatitis
When you start to prevent the development of chronic prostatitis, you should know:
- The risk of developing the disease increases over the years.
- Representatives of the Negroid race are more prone to disease.
- A familial predisposition to the disease is not excluded.
People with a predisposition to develop chronic prostatitis should be more attentive to their health condition.
Disease prevention tips:
- Drink plenty of fluids. Frequent urination promotes drainage of microflora from the urethra.
- Prevent diarrhea and constipation.
- Eat a balanced diet. Avoid eating foods high in saturated carbohydrates and fats, which can lead to weight gain.
- You should limit the use of substances that irritate the urethra as much as possible: spicy and spicy foods, smoked meats, sauces and spices, coffee and alcohol.
- Stop smoking. Nicotine negatively affects the condition of the walls of blood vessels.
- Do not get too cold.
- Do not hold the bladder empty.
- Make an active lifestyle, exercise. Exercise to strengthen the pelvic floor muscles, which can eliminate venous congestion, which in turn supports the normal functioning of the prostate.
- Have a regular sex life. Avoid prolonged abstinence. The gland should be released immediately from the secretion.
- Stay in a monogamous relationship. Indiscriminate sex increases the likelihood of acquiring sexually transmitted diseases.
- If you have complaints from the genitourinary organs, contact your urologist immediately.
